Naturopathic Sexology
Naturopathic Sexology
 Naturopathic Sexology
Naturopathic SexologySex therapy is the treatment of sexual dysfunction, such as non-consummation, premature ejaculation or erectile dysfunction, low libido, unwanted sexual fetishes, sexual addiction, painful sex or lack of sexual confidence, assisting people who are recovering from sexual assault, problems commonly caused by stress, tiredness and other environmental and relationship factors. Sex therapists assist those experiencing problems in overcoming them, in doing so possibly regaining an active sex life.
Sexual dysfunction or sexual malfunction (see also sexual function) is difficulty during any stage of the sexual act (which includes desire, arousal, orgasm, and resolution) that prevents the individual or couple from enjoying sexual activity.
Dr. Georgiou is a qualified Clinical Sexologist as well as a Naturopath and has developed a method of treating these sexual problems that is rather unique in that it combines both the traditional treatment protocols of sex therapy using cognitive-behavioral approaches, with naturopathic approaches that are very effective at treating the physical or organic causes that include circulatory problems in the case of erectile problems, etc. This approach he has termed NATUROPATHIC SEXOLOGY, a completely new approach that is nowhere to be found on Google (try searching and you will be brought back to this site only)! He has also developed a Diploma course in Naturopathic Sexology too.
 Combining these two very powerful treatment methods, now known as Naturopathic Sexology, has helped to increase the probability of success, and the Center enjoys a very high success rate approaching 90% with the majority of sexual problems.
Combining these two very powerful treatment methods, now known as Naturopathic Sexology, has helped to increase the probability of success, and the Center enjoys a very high success rate approaching 90% with the majority of sexual problems.
Emotional factors affecting sex include both interpersonal problems (such as marital/relationship problems, or lack of trust and open communication between partners) and psychological problems within the individual (depression, sexual fears or guilt, past sexual trauma, sexual disorders, and so on).
Physical factors include drugs (alcohol, nicotine, narcotics, stimulants, antihypertensives, antihistamines, and some psychotropic drugs); injuries to the back, problems with an enlarged prostate gland, problems with blood supply, nerve damage (as in spinal cord injuries); or disease (diabetic neuropathy, multiple sclerosis, tumors, and, rarely, tertiary syphilis); failure of various organ systems (such as the heart and lungs); endocrine disorders (thyroid, pituitary, or adrenal gland problems); hormonal deficiencies (low testosterone, estrogen, or androgens); and some birth defects.
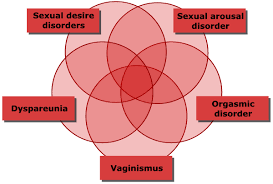
Sexual dysfunction disorders are generally classified into four categories: sexual desire disorders, sexual arousal disorders, orgasm disorders, and sexual pain disorders.
 1.Sexual desire disorders or decreased libido can be caused by a decrease in normal estrogen (in women) or testosterone (in both men and women) production. Other causes may be aging, fatigue, pregnancy, medications (such as the SSRIs) or psychiatric conditions, such as depression and anxiety. Loss of libido from SSRIs usually reverses after SSRIs are discontinued, but in some cases it does not. This has been called PSSD; however, this is not a classification that would be found in any current medical text.
1.Sexual desire disorders or decreased libido can be caused by a decrease in normal estrogen (in women) or testosterone (in both men and women) production. Other causes may be aging, fatigue, pregnancy, medications (such as the SSRIs) or psychiatric conditions, such as depression and anxiety. Loss of libido from SSRIs usually reverses after SSRIs are discontinued, but in some cases it does not. This has been called PSSD; however, this is not a classification that would be found in any current medical text.
2.Sexual arousal disorders were previously known as frigidity in women and impotence in men, though these have now been replaced with less judgmental terms. Impotence is now known as erectile dysfunction, and frigidity has been replaced with a number of terms describing specific problems with, for example, desire or arousal.
For both men and women, these conditions can manifest as an aversion to, and avoidance of, sexual contact with a partner. In men, there may be partial or complete failure to attain or maintain an erection, or a lack of sexual excitement and pleasure in sexual activity.
There may be medical causes to these disorders, such as decreased blood flow or lack of vaginal lubrication. Chronic disease can also contribute, as well as the nature of the relationship between the partners. As the success of sildenafil (Viagra) attests, most erectile disorders in men are primarily physical, not psychological conditions.
 3.Orgasm disorders are a persistent delay or absence of orgasm following a normal sexual excitement phase. The disorder can occur in both women and men. Again, the SSRI antidepressants are frequent culprits — these can delay the achievement of orgasm or eliminate it entirely. Premature ejaculation is also another commonly occuring problem.
3.Orgasm disorders are a persistent delay or absence of orgasm following a normal sexual excitement phase. The disorder can occur in both women and men. Again, the SSRI antidepressants are frequent culprits — these can delay the achievement of orgasm or eliminate it entirely. Premature ejaculation is also another commonly occuring problem.
4.Sexual pain disorders affect women almost exclusively and are known as dyspareunia (painful intercourse) and vaginismus (an involuntary spasm of the muscles of the vaginal wall that interferes with intercourse). Dyspareunia may be caused by insufficient lubrication (vaginal dryness) in women.
Poor lubrication may result from insufficient excitement and stimulation, or from hormonal changes caused by menopause, pregnancy, or breast-feeding. Irritation from contraceptive creams and foams can also cause dryness, as can fear and anxiety about sex.
It is unclear exactly what causes vaginismus, but it is thought that past sexual trauma (such as rape or abuse) may play a role. Another female sexual pain disorder is called vulvodynia or vulvar vestibulitis. In this condition, women experience burning pain during sex which seems to be related to problems with the skin in the vulvar and vaginal areas. The cause is unknown.
Sexual dysfunctions are more common in the early adult years, with the majority of people seeking care for such conditions during their late twenties through thirties. The incidence increases again in the geriatric population, typically with gradual onset of symptoms that are associated most commonly with medical causes of sexual dysfunction.
Sexual dysfunction is more common in people who abuse alcohol and drugs. It is also more likely in people suffering from diabetes and degenerative neurological disorders. Ongoing psychological problems, difficulty maintaining relationships or chronic disharmony with the current sexual partner can also interfere with sexual function.
Dr Georgiou has a Ph.D in Clinical Sexology and is also a Clinical Psychologist, Naturopath and has an additional Doctor of Science in Alternative Medicine. He is a member of:
- Chartered Psychologist, UK, BPS (C.Psychol)
- Diplomate of the American Board of Sexology, USA (ABS)
- Registered Sex Therapist with ABS, USA
- The American College of Sexologists, USA (ACS)
- Fellow of the American Academy of Clinical Sexologists, USA (FAACS
- The General Council and Register of Naturopaths, UK (GCRN)
- The Institute of Biology, UK (MIBiol)
Videos to Watch:
Human Sexuality: What Do We Know?

Contact us or book an appointment now.