Health Benefits of Full Spectrum Light
Good health can be maintained and many disease conditions alleviated with adequate exposure to full-spectrum light. Read about the health benefits of full spectrum light.
America has a phobia, an irrational fear, about ultraviolet (UV) light. In a new science fad, unwise practices are being urged on us. The resulting sickness and misbehaviour will mystify yet enrich physicians, psychiatrists, dentists and criminal specialists as well as pharmaceutical drug companies.In too many scientific and medical fields, for a lot of researchers the truth is defined only in relationship to the next grant, peer pressure and the fight to further an entrenched view. This essentially political process goes on despite any–in this case very strong–evidence to the contrary.1 Much “science” research is known to be fraudulent.2, 3 Such a flow of funded research almost exclusively in one direction is characteristic of potentially dangerous science fads. Almost all “scientists” are out to prove something so as to continue their careers; to them, finding the truth is only secondary.UV intensity is now forecast in population centres daily. The US Environmental Protection Agency (EPA) suggests that when outdoors we should “protect ourselves against ultraviolet light whenever we can see our shadow”. And many physicians give their patients the same warning. This is terrible advice. If man were a machine, a doctor could repair or replace one part without worrying about the rest of the contraption. Man is no machine, but more like a web or hologram. Every organ and every part affects all the other parts; in fact, cells in every part communicate with all the other parts.4As a result of the EPA’s kind of advice, which is based on junk science, the use of sunglasses is epidemic; we hide behind stylish darkened car windows, we slather our skin with sunscreen for even brief sun exposure. People who engage in these practices are ruining their disposition5 and health.The phobia arose after investigators anaesthetised animals, propped their eyes open and shined intense UV light into them; this damaged their retinas. Excessive exposure to one kind of ultraviolet (shorter-wave, germicidal UVC) can damage tissue. But the EPA makes the ridiculous leap from that truth to the conclusion that we should avoid all UV. UVC is not present increasingly in sunlight; a purported thinning of the protective ozone layer has been debunked (see below). UVC is found in tanning salons and halogen lamps.6 In fact, the trace amounts of UV radiation in natural daylight are required for physical and mental health, civilised behaviour, muscle strength, energy and learning.7 Sunlight, in moderation, improves immunity and stimulates our metabolism while decreasing food craving, and increases our intelligence.Ozone Hole Danger Disproved
The following passages and references are from Richard Hobday’s book, The Healing Sun: Sunlight and Health in the 21st Century.8
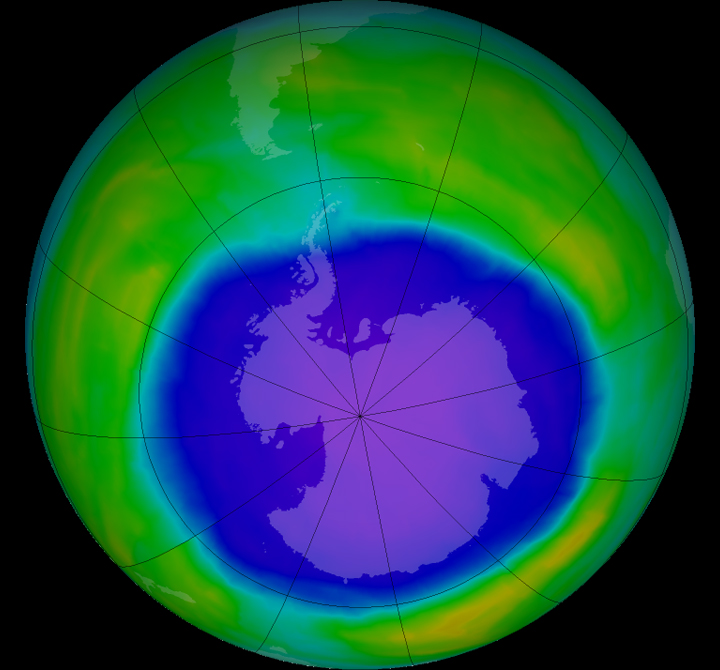 “There have been no increases in skin cancer, eye diseases, immune system disorders or environmental damage which can be attributed to an increase in ultraviolet radiation. The largest South American city close to the Antarctic ozone hole is Punta Arenas in southern Chile. Despite reports to the contrary, there have been no ozone-related health problems at Punta Arenas, and measurements of ultraviolet radiation show that any increases are too small to have any appreciable effect.[9]
“There have been no increases in skin cancer, eye diseases, immune system disorders or environmental damage which can be attributed to an increase in ultraviolet radiation. The largest South American city close to the Antarctic ozone hole is Punta Arenas in southern Chile. Despite reports to the contrary, there have been no ozone-related health problems at Punta Arenas, and measurements of ultraviolet radiation show that any increases are too small to have any appreciable effect.[9]
“A paper published in 1998 by the European Science and Environmental Forum challenges the consensus view on ozone depletion, and argues that predictions made by the scientific establishment and the media have been ill-founded.[10] If this is the case, and the hole in the ozone layer is, after all, a temporary thinning of the upper atmosphere in the early spring, then there is no reason to fear that people will develop skin cancer because ultraviolet radiation has become more dangerous.
“There is certainly no evidence to support the widely held view that the increase in malignant melanoma in recent years is in some way linked to ozone depletion. The trend predates the issue of ozone loss, which may have been going on for some time before it was noticed. A paper published in the British Journal of Cancer shows that from 1957 to 1984 the incidence of malignant melanoma in Norway increased by 350 per cent for men and 440 per cent for women. During the same period there was no change in ozone levels over Norway, nor any significant change in annual exposure to ultraviolet radiation from the Sun.[11] Scare stories, such as the one about sheep in Chile developing cataracts because of increased ultraviolet radiation, are not supported in the scientific literature. The sheep in question were later found to have had an infectious disease, and sunlight was not implicated.[12, 13]
“What is clear, however, is that there is a great deal of ill-informed comment on the subject of ozone depletion and, for that matter, sunbathing. Should depletion of the ozone layer ever become a cause for real concern, then some people might develop cancer who might not have, had there been no depletion, but until this happens there is much more to be gained from investigating the real causes of skin cancer and encouraging safe sunbathing than in being preoccupied with the state of the Earth’s upper atmosphere and blaming everything on the Sun. Diet and lifestyle play a far more significant part in the genesis of cancer than is currently recognised. The same can also be said about another condition that is supposed to be on the increase because of ozone depletion–that of senile cataract.”
Note that even low exposure to UVB significantly increases the risk of cataracts,14 but only with the consumption of a Western junk food diet rich in unsaturated fats and their oxidised products.15, 16 Those (including myself) who consume a more sensible diet, and supplement it with vitamins C and E, do not get cataracts even from lengthy sun exposure.17, 18
PHOTOBIOLOGY
Starting from a high-school hobby of time-lapse photography, the late John N. Ott, DScHon,19 founded the new science of photobiology. He was active into his tenth decade.
Dr Ott’s last book, one of many publications, is Light, Radiation and You: How to Stay Healthy (1990).20 In it he wrote: “Mankind adapted to the full range of the solar spectrum, and artificial distortions of that spectrum–malillumination, a condition analogous to malnutrition–may have biologic effects.” In an interview published in 1991, he noted: “There are neurochemical channels from the retina to the pineal and pituitary glands, the master glands of the whole endocrine system that controls the production and release of hormones. This regulates your body chemistry and its growth, all organs of your body, including your brain, and how they function.”21
The critical reader will ask: where are the controlled, scientific tests supporting Dr Ott’s statements? The answer to that question is: who can make money promoting sunlight? Think about it.
SIDEBAR
Two hours of bright light in the evening can sometimes cure symptoms such as weight gain, depression, carbohydrate craving, social withdrawal, fatigue and irritability.22
I. Ultraviolet Deprivation Health Effects
First, let’s consider the health effects of ultraviolet deprivation.
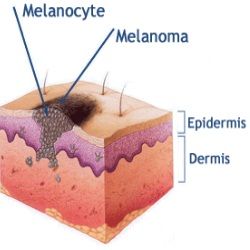
Indoor Lighting and Melanoma
Malignant melanoma is often alarmingly but wrongly blamed on sun exposure. The dangerous kind, called skin cancer, is ultimately fatal if not corrected. A study by the US Navy found the most melanoma in people who worked indoors all the time. Those who worked both outdoors and indoors some of the time had the lowest incidence. Also, most melanomas appeared on parts of the body that are seldom exposed to sunlight.23 The inference is that both very high and very low exposures to UV light can be harmful–and moderate exposure is healthful.24
Sunscreens and Melanoma
 Sunscreens block out only UVA and UVB, which we all need in trace amounts, but not the potentially dangerous, germicidal UVC. No commercial sunscreens have been proved safe.25 Their chemicals penetrate the skin into the circulation and add to the burden of toxins to be detoxified.26 Commercial sunscreens increase the risk of melanoma by causing mutations when the cells’ chromosomes interact with the chemicals and the light.27 Natural sunscreens, as well as commercial ones, curtail needed uptake of vitamin D3 from UVB, increasing the risk of the bone-thinning disease osteoporosis.
Sunscreens block out only UVA and UVB, which we all need in trace amounts, but not the potentially dangerous, germicidal UVC. No commercial sunscreens have been proved safe.25 Their chemicals penetrate the skin into the circulation and add to the burden of toxins to be detoxified.26 Commercial sunscreens increase the risk of melanoma by causing mutations when the cells’ chromosomes interact with the chemicals and the light.27 Natural sunscreens, as well as commercial ones, curtail needed uptake of vitamin D3 from UVB, increasing the risk of the bone-thinning disease osteoporosis.
Moreover, Lita Lee, PhD, notes: “Mounting evidence indicates that many of them [sunscreens] contain carcinogens and that the rise of skin cancers parallels the increase in sunscreen usage. The only sunscreen I recommend is coconut oil, although, believe me, you cannot slather this oil on your skin and bake in the sun all day. Adding a little iodine to the coconut oil for the first week of summer gives added protection; however, do not use the iodine for more than a week, as continued use will inhibit your thyroid function. In my opinion, the only other safe (non-carcinogenic) sunscreen would be one containing titanium dioxide.”28
Fluorescent Lighting and Melanoma
A study published in the prestigious medical journal Lancet and a Russian study found that fluorescent light rather than sunlight promotes melanoma, proportionately to the time of exposure.29, 30 In the Lancet study, among a sample of nearly 900 women, those who worked indoors under fluorescent lighting had 2.l times higher melanoma risk (95% confidence interval, CI, 1.32 to 3.32) than others. Among women exposed for 20 years or more, the relative risk (RR) was 2.6 (95% CI, 1.2 to 5.9). Relative risks were lower in women who had been most heavily exposed to sunlight, both playing outdoors as children and sunbathing as adults. In a smaller sample of men, the RR for fluorescent lights with 10 or more years’ exposure was 4.4; and for those who had spent the least time in the sun while children, the RR was 7.3.
And so we see that lengthy exposure to full-spectrum sunlight, including trace UV, partially “immunised” both men and women against later development of melanoma. These exposures had taken place in the 1960s and 1970s, before the supposed thinning of the protective ozone layer far above us. But as we saw earlier, UV penetration of the atmosphere has not increased.31, 32
All this thoroughly explodes the claim that sun exposure causes malignant melanoma.
In the 19 years since publication of Beral’s carefully researched article in the Lancet, no one has refuted the finding. But many ignore it and could make more money if the article and its information would simply go away.
Why do fluorescent lights cause melanoma? “Emissions from such light extend into the potentially carcinogenic range.”33
Dr Ott found that, specifically, the cathodes located at the ends of the light tubes emit X-rays and other electromagnetic pollution. Plants living under the central portion of long fluorescent light tubes grow normally; but when placed close to the ends of the tubes, their growth is abnormal and stunted. Laboratory animals placed in a cage close to the ends of these light tubes become aggressive and cannibalistic.
Dr Ott also found that the light from fluorescent tubes, as well as TV sets and computer terminals, causes red blood cells to clump together after prolonged exposure. This reduces alertness, promotes a tired feeling and increases the risk of heart attack and stroke.34 But when the ends of the light tubes are shielded with lead and traces of UV are added to the light, plants and animals under them grow and function normally.35 And so wrapping the ends of fluorescent light tubes with lead tape, says Dr Ott, is fully as important as full-spectrum light itself.36
Melanoma can also result from excessive exposure to sunlamps;37 their rays and those from bright halogen lights include some of the dangerous UVC.38 If users of sunlamps consume a junk diet, their risk of melanoma will be increased. Halogen lamps are also a serious fire hazard if they fall over or if inflammable material touches the extremely hot bulb.39, [40]
Sidebar
Valdemar Valerian, PhD, and his Leading Edge Research Group “…noticed that DNA molecules undergo erratic vibrational patterns in the vicinity of cathode ray tubes (television or computer monitors), and that a certain subsonic signal emanating from computer monitors connected to the Internet make the DNA molecules vibrate in unison, in a form of entrained pattern. We consulted the eminent Russian researcher Professor D. S. Goldstein. He said: ‘I know that. It is a phenomenon known as electronically induced sonochemistry. That is how mutations occur, and that is why I stay away from the Internet.’ “40
Chlorination and Melanoma
Drinking and swimming in chlorinated water can also cause malignant melanoma.41, 42, 43, 44 Sodium hypochlorite, used in chlorination of water for swimming pools, is mutagenic45 in the Ames test and other mutagenicity tests.46, 47 Redheads and blonds are disproportionately melanoma-prone; their skin contains a relative excess of pheomelanins48 compared to darker people.49
Franz H. Rampen and his associates in The Netherlands state that the worldwide pollution of rivers and oceans and the chlorination of swimming pool water have promoted an increase in melanoma.50, 51, 52
Another major factor in the increase in reported incidence of melanoma has been physicians’ continually relaxing their standards for what constitutes melanoma.
Synthetic Hormones and Melanoma
What about oral contraceptives and hormone replacement therapy (HRT)? Melanomas have increased sharply among women in the principal Pill-taking countries of Australia, America and in Europe. In the Walnut Creek (California) study, all the women who developed melanomas under the age of 40 had used the Pill. By 1981, the overall increased melanoma risk for Pill-users was statistically significant at three times.53 The Pill also promotes development of heart attacks, in part by depleting body stores of vitamin B6.54
Further, like breast cancer cells, those tumours have oestrogen receptors. And so women on HRT are more likely to develop melanomas than non-users. A recent study of 52,705 women on HRT found that the risk of breast cancer increases by 2.3 per cent for each of the 11 years the average woman takes HRT. The good news is that the effect diminishes on stopping it and disappears after about five years. The authors comment: “These findings should be considered in the context of the benefits and other risks associated with the use of HRT.”55 Others challenge the assumption that HRT provides benefits.56, 57, 58
II. Ultraviolet Deprivation Health Effects
Certain effects of ultraviolet deprivation are equally remarkable and tie together with health benefits.
FS Light & Childhood Health
 In 1973, radiation-shielded full-spectrum (FS) lights were installed in five classrooms in Sarasota, Florida. And what happened? Several extremely hyperactive, learning-disabled children calmed down completely and learned to read. Absenteeism dropped. The children in four standard-lit rooms continued to misbehave (as tracked by concealed motion-detecting cameras); their learning disabilities and absenteeism were unabated.59 And after a year, students in the full-spectrum classrooms had one-third less tooth decay than those taught under standard lighting. Laboratory mice, which had been exposed all their waking hours to FS light, had zero tooth decay.60 Similar findings were reported from California, Washington state and Alberta, Canada.61 A classroom comparison in Vermont found that full-spectrum lighting strengthened immunity.62, 63
In 1973, radiation-shielded full-spectrum (FS) lights were installed in five classrooms in Sarasota, Florida. And what happened? Several extremely hyperactive, learning-disabled children calmed down completely and learned to read. Absenteeism dropped. The children in four standard-lit rooms continued to misbehave (as tracked by concealed motion-detecting cameras); their learning disabilities and absenteeism were unabated.59 And after a year, students in the full-spectrum classrooms had one-third less tooth decay than those taught under standard lighting. Laboratory mice, which had been exposed all their waking hours to FS light, had zero tooth decay.60 Similar findings were reported from California, Washington state and Alberta, Canada.61 A classroom comparison in Vermont found that full-spectrum lighting strengthened immunity.62, 63
Why was there so much less tooth decay after exposure to full-spectrum light, including trace UV? And why did immunity improve under FS lights? According to Dr Ott: “Every nutritional substance and medicine has a specific wavelength absorption. If those wavelengths are missing in the artificial light source a person is exposed to, then the nutritional or other hoped-for benefits of the substance will not be utilised.”63a UV functions as a nutrient and as a co-factor (a substance required for a bodily process to occur) in the utilisation of other nutrients.
So the full-spectrum lights corrected the children’s deficiency of vitamin D3 (not the same as the toxic form of vitamin D added to milk), now considered a pro-hormone. This enabled more complete calcium absorption–and lowers the risk of osteoporosis and hip fractures in later life. Recent research has found that nearly half the people of all age groups taking RDA-strength supplements have too little vitamin D. When the body doesn’t have enough of it to absorb adequate calcium from food, it extracts calcium from bone.64
FS light also strengthens immunity in other ways. It helps protect against multiple sclerosis, heart attacks and conversion of HIV to AIDS, among other things. These are elaborated and fully referenced in the remainder of the paper [see NEXUS website]. “Protect ourselves from ultraviolet whenever we can see our shadow,” as the EPA frighteningly warns? Won’t doing that then constitute a full-employment plan for dentists, orthopaedic surgeons and oncologists as well as pharmaceutical drug companies?
FS Light vs Cancers
Cancers hate full-spectrum light. A tumour-susceptible strain of mice lived more than twice as long under full-spectrum as under standard lighting, and rats exposed to full-spectrum light had significantly lessened tumour development.65 The tunnel-visioned National Cancer Institute and American Cancer Society ignore these findings, which six major medical centres have confirmed.66
Terminal cancer patients, who Dr Ott knew of personally, got well in a rocking chair in the sunshine. Dr Jane Wright, directing cancer research at Bellevue Memorial Medical Center in New York City in 1959, was fascinated by Ott’s ideas. So she instructed progressive-tumour patients to avoid artificial lights and stay outdoors as much as possible that summer. They were not to wear sunglasses or prescription lenses, which block UV light. By that fall, the tumours in 14 of 15 had not grown, and some patients had got better; the one whose condition deteriorated sat outdoors but wore prescription lenses. Ott has been criticised for making no scientifically controlled human studies. Well, funding for continuation of that study was withdrawn–that was his experience over and over.67
One woman with cancer ventured out with Norwegian fishermen, ate a lot of their catch and recovered; friends ate fish but stayed inside–and their cancers killed them.68 Had she “protected” herself from UV when she could see her shadow, as the EPA advises, would her cancer have ended? And if sun-loving Arizonans threw away their sunscreens and sunglasses and limited their sun exposure to about 30 minutes a day,69, 70 wouldn’t their cancers largely disappear?
A Chicago-area elementary school suddenly reported five times the national average incidence of leukaemia, a kind of cancer of the blood. All of the afflicted children but one were being taught in rooms where teachers kept the blinds drawn, and the children were exposed all day only to melanoma-promoting fluorescent light. When even the amount of UV that can get through window glass was let in, the leukaemia cluster disappeared.71 (Raymond Peat, PhD, thinks FS sunlight is best received through glass.72)
FS Light vs Arthritis and Blindness
Early in his research career, Dr Ott fell and broke his glasses; soon, his arthritis disappeared. And in 1996, Marion Patricia Connolly, executive director of Price&endash;Pottenger Nutrition Foundation (PPNF), had much the same experience. Full-spectrum eyeglasses, i.e., lenses that transmit all ultraviolet light, are difficult to find. I take off my glasses outdoors whenever I can.
Exposed to full-spectrum light, a father rat is docile and even helpful after his babies are born. But when the same rat pair is moved under standard light, before the birth of the next litter the male must be removed to prevent aggressiveness and cannibalism. Moved back to natural light for still another litter, he is gentle again.73 Although human fathers aren’t likely to eat their babies, do we really want more domestic aggressiveness?
Alternating full-spectrum light and total dark cured children born blind as a result of brain injury. The technique was advocated by W. H. Bates about 1904 and endorsed by Aldous Huxley in 1930. Efficacy was confirmed in the recent Annual Report from the British Institute for Brain Injured Children.74
How can all this be explained? Full-spectrum light, entering the eyes during waking hours, promotes night-time pineal gland secretion of melatonin. This sleep-promoting antioxidant destroys carcinogenic hydroxyl radicals–and also slows ageing.75, 76 Melatonin can suppress growth of human breast cancer cells in vitro (in a test tube), and can cross all barriers to enter every cell.77, 78 So enough sleep–best achieved in total darkness79–becomes anti-ageing, antioxidant, anti-cancer, anti-heart attack therapy!
Except in short-term emergencies, people younger than about 50 should use supplements of melatonin cautiously, if at all.80 For people over 40 to 45, one to three milligrams before bedtime safely promotes both prompt falling asleep and a good night’s rest, in addition to its other benefits.81
In a laboratory, viruses are weakened by exposure to full-spectrum light that includes traces of UV. Infectious organisms such as E. coli K12 AB2480, which can cause food poisoning, dislike ultraviolet too.82 The Morris Center in Winnipeg, Canada, promotes “amazing” healing by shining full-spectrum light onto wounds.83
FS Light vs Seasonal Affective Disorder
The power of full-spectrum light against SAD (seasonal depression)–again, by entering the eyes–has been amply demonstrated. FS light benefits nonseasonal depression, too,84 but not as much.85 Such light energises and regulates the body’s entire chemistry. Won’t “protecting” millions of people from UV, as the EPA advocates, then worsen the growing epidemic of depression?
Dietary sufficiency of vitamin D also needs consideration here. “Seasonal affective disorder has been treated successfully with vitamin D. In a recent study covering 30 days of treatment comparing vitamin D supplementation with two-hour daily use of light boxes, depression completely resolved in the D group but not in the light-box group.”87
The cells in the retinas of your eyes will not divide and regenerate without a small amount of ultraviolet light. And so full-spectrum light reduces the risk of retinal degeneration, the leading cause of blindness among the elderly.88 Retinal haemorrhage, the most severe phase of the condition, can also result from long-term use of aspirin.89 (A prominent ophthalmologist declared the outcome “unlikely”; however, an exhaustive computer literature search by Kirk Hamilton, PA-C, publisher of Clinical Pearls News, found no refutation of the finding.) White willow bark provides the same benefits as aspirin without stomach irritation or blindness, as do three glasses daily of purple grape juice. And unlike aspirin,90 the flavonoids in purple grape juice remain effective when adrenaline levels rise.91 Two 400-milligram capsules of white willow bark are equivalent to one baby aspirin.92 Eating a lot of dark-green leafy vegetables such as spinach,93 kale and Brussels sprouts also helps avoid this condition.94, 95
Many dermatologists advise older patients to stay out of the sun to avoid skin cancer. The thousands of elderly patients rotting in nursing homes come to mind. That advice may unintentionally help to make patients sicker and older beyond their years. Staying indoors will cause problems a lot worse than skin cancer. Older people’s bones will crumble and break (osteoporosis); these elderly patients will hate living (depression). Articles in the journals Cancer, Cancer Research and Preventive Medicine suggest that avoiding sunlight could promote the development of cancers other than those of the skin.96, 97, 98
FS Light vs Neurological Diseases
Research by Reuven Sandyk, MD, who practises medicine in Connecticut, shows that long-term deprivation from sunlight exposure increases the risk of multiple sclerosis and Parkinson’s disease through depressed secretion of the hormone melatonin by the brain’s pineal gland. This appears to explain the south-north gradient in the incidence of MS: the farther from the equator, the more common it is.99 All the MS patients he tested had extremely low melatonin levels and their pineal glands were calcified, or hardened.
Reduction in melatonin secretion, he found, may be associated with zinc deficiency in ADHD (attention deficit hyperactivity disorder).100 “Since melatonin stimulates serotonin synthesis,[101] and serotonin deficiency has been linked to aggressive behaviour,[102] it is possible that a high prevalence of conduct disorder and aggressive behaviour in ADHD patients could be related to reduced melatonin and serotonin associated with (but not caused by) zinc deficiency.[103]”
Dr Sandyk applies extremely weak alternating-current fields to the brain; this stimulates melatonin secretion, bringing about remarkable subjective and objective improvement of MS and Parkinson’s patients within one to two minutes. The magnetic field he uses is at 2 to 7 hertz (vibrations per second), a physiological frequency, i.e., near the rate used by brain neurotransmitters.
Melatonin destroys carcinogenic hydroxyl radicals by neutralising their precursor molecules, and so it should help against Parkinson’s and Alzheimer’s diseases.104 Melatonin interferes with oestrogen receptor sites on cells; excessive oestrogen from the Pill and from HRT causes breast cells to hyperproliferate (become cancerous), and melatonin blocks this action.105 It also slows senescence.106 The decline in its levels in everyone’s bodies owing to longer daily exposure to light has been suggested as one possible factor explaining the continual spread of cancer in the 20th century.107, 108 Some of Dr Sandyk’s patients with Alzheimer’s disease, migraine and pain syndromes also benefit from exposure to such magnetic fields–suggesting that sunlight deprivation may contribute to the aetiology of those distressing illnesses.109
FS Light vs CHD and Infections
Staying completely out of the sun may also increase the risk of heart attacks and much more by another route. David Grimes, MD, at Blackburn Royal Infirmary in Blackburn, UK, notes that heart attacks are commonest in the parts of the world–such as northwest United Kingdom–that have the least sunshine. And Asian populations in the British Isles have a particularly high risk of death from heart attack that cannot be explained on dietary grounds. Having come from countries in which the sun is so strong that exposure must be minimised, they have a cultural tendency to avoid the sun.
Dr Grimes traces causation of many cases of CHD (coronary heart disease) to the microbe Chlamydia pneumoniae and low immunocompetence from too low a level of vitamin D among those avoiding sunshine. Sunlight could determine whether squalene, the precursor to both vitamin D and cholesterol, converts into vitamin D (in the presence of enough sunshine) or into excessive cholesterol (if sunlight is deficient.)110 A deficiency of vitamin B6 promotes infection, e.g. by H. pylori and Chlamydia, as one of its mechanisms of increasing risk of heart attack.111, 112
Dr Grimes links respiratory infections and chronic bronchitis, called “the English Disease”, to poor immunocompetence due to sunlight deficiency, worsened by cigarette smoking. (In southern Europe, smoking rates are much higher, but recurrent respiratory tract infections are scarce.) Glasgow, Scotland, has high rates of osteomalacia and rickets, which he says are definitely the result of sunlight deficiency. Dr F. A. Spencer has noted a higher incidence of heart attacks in winter; he has related this to low levels of vitamin D and to depression from the winter months.113
Also, Crohn’s disease (regional enteritis or intestinal irritation) is much more common in cloudy northwest England than in sunny southern Europe–that is, if we accept that Crohn’s is a microbial disease, as current research confirms, probably due to Mycobacterium paratuberculosis. Once again, sunlight in the Mediterranean area could be protective through immuno-enhancement.114
There are other risks. An Alabama researcher found that lack of enough sunshine exposure may increase the risk of hypertension in blacks and other dark-skinned people. Those with greater amounts of pigment in the skin require six times the amount of ultraviolet B (UVB) light to produce the same amount of vitamin D3 found in lighter-skinned people.115 And Dr Esther John of Northern California Cancer Center reported that daily exposure to sunshine, without sunscreen, appears to lessen the risk of breast cancer.116
Addendum I
Skin Cancers
What about skin cancers? One was taken off my nose in 1989, and another in 1997; such skin cancers are totally harmless if removed promptly. Recent research has found at least two ways to minimise even that occasional inconvenience, and these offer other major benefits:

(a) Drink lots of green tea. In one study, cancer-sensitive mice were pre-treated with a strong carcinogen; their only source of liquid, green tea, lowered keratoacanthomas and carcinomas by 65 to 90 per cent. Decaffeinated tea has been found to be nearly as effective as plain.117 Applying green tea to the skin was equally effective against tumour formation from a carcinogen or intense UV light.118 And in an animal tumour model, green tea ingredients induced apoptosis (programmed cell death “for the good of the organism”) among cancer cells.119
Recent research has found that tea can be high in fluoride. The tea plants grow best on fluoride-rich soil and can suck up the chemical from dumped fluoride as well. This fluoride is toxic and can weaken thyroid function.119a
The bioflavonoids–flavone compounds that accompany vitamin C in plant structures120–in green tea help prevent cancers, cardiovascular and liver diseases as well as keratoses.121 And they explain why green tea is nearly 20 times stronger an antioxidant than vitamin E in the alpha-tocopherol form.122
(b) Eat a diet low in trans- fats, supplemented by fresh, organic, refrigerated flaxseed and cod liver oils for omega-3 essential fatty acids (EFAs).
One hears warnings of glaucoma (excessive pressure in and hardening of eyeballs) from sun exposure. That is a risk if you eat a processed-food diet. The EFAs are largely lacking in low-fat Western diets, including the US Department of Agriculture’s “food pyramid”. Among many other health benefits, omega-3 EFAs regulate eye pressure.
Glaucoma can also result from the use of inhaled steroids for treating asthma. For many older patients, inhaled steroids intended to block or reduce inflammation, and formerly claimed not to circulate throughout the system, promote glaucoma–the leading cause of blindness–and cataracts. In a comparative study, the glaucoma risk appeared to be elevated by 44 per cent compared to matched patients not using inhaled steroids. Lea Davies of Georgetown University Medical Center in Washington, DC, adds that inhaled steroids may cause about one-third of the 3,000 glaucoma cases developing each year among Americans over the age of sixty-five.123 Also, a published clinical test showed that melatonin offers still another benefit: it lowers eyeball pressure in glaucoma patients–and the insomnia age group, for whom its use is safe and appropriate, is the same as the glaucoma age group.124 Flaxseed oil is best taken with 400 international units (IUs) of antioxidant vitamin E,125, 126 which should include the other members of the natural-source tocopherol complex as well as the d-alpha part.127 Germany’s late Johanna Budwig, PhD, developer of this therapy,128 was nominated seven times for a Nobel Prize and continued activity into her tenth decade of life. How much flax oil? Healthy people should have one to three teaspoonfuls a day, either out of a spoon or in food, e.g., on salads (the oil must have a pleasant, nutty flavour). And sick people? In her books, Dr Budwig told of hundreds who recovered from cancer, diabetes, lupus, bronchial spasms, Hodgkin’s disease, atherosclerosis, stomach ulcers, prostate disease, arthritis, eczema and immune deficiency syndromes including multiple sclerosis. They accomplished these healing miracles by taking three tablespoonfuls of flax oil a day with unpasteurised cottage cheese to improve absorption. The benefits of this diet can be strengthened by resveratrol, another bioflavonoid found in grapes and other natural foods.129
No one is interested in paying for a controlled trial of flaxseed oil therapy. Its successful proof and wide use would destroy much of medical practice and the pharmaceutical drug industry as well as the careers of the researchers involved and the editor of any journal that published the findings. And since medical journals rely on hundreds of millions of dollars yearly in revenues for advertising from pharmaceutical drug companies, the journal itself would be out of business in 10 minutes.
Raymond Peat, PhD (chemistry), a world authority, has shown that coconut oil, consumed in the diet at an ounce [29.6 cc] or more per day, enables the body to generate ample essential fatty acids (also see below). He also warns that supplemented EFAs can weaken immunity and actually poison the body; they are deliberately used in organ transplantation to minimise risk of rejection by the recipient’s immune system.130
Addendum II
Selenium supplements
 Supplemented selenium (Se) at 50 to 250 micrograms daily protects the skin against damage from excess sun exposure.131 (Intakes above 250 mcg, which could be toxic, should be used only for short periods under the guidance of a knowledgeable practitioner.) Two grams a day of vitamin C, taken together with 1,000 IU of vitamin E, also protects against sunburn.132
Supplemented selenium (Se) at 50 to 250 micrograms daily protects the skin against damage from excess sun exposure.131 (Intakes above 250 mcg, which could be toxic, should be used only for short periods under the guidance of a knowledgeable practitioner.) Two grams a day of vitamin C, taken together with 1,000 IU of vitamin E, also protects against sunburn.132
Hardly anyone will experience skin damage from our suggested 20 to 30 minutes’ daily sun exposure. But the selenium supplement is worth taking on its other merits, which are extremely important:
(a) A massive scientific/medical literature supports selenium’s efficacy against cancer and cardiovascular disease (CVD). A map of the United States showing areas of low soil selenium almost perfectly matches maps showing the areas of highest incidence of both cancer and CVD. The same is true in New Zealand and Australia.133 Crib death (cot death, or SIDS, sudden infant death syndrome) is also more common in areas of low soil selenium, such as in America’s Pacific Northwest and parts of New Zealand.134 (See also Dr Lendon Smith’s and my work on SIDS.135, 136)
(b) More than 10 papers published in the past two years relate declining selenium levels to the progression of HIV (human immunodeficiency virus) disease. An article in the Journal of AIDS (September 30, 1997) found that patients deficient in Se are almost 20 times more likely to die of causes related to HIV than are people with enough Se.
Recent research has discovered that selenium at 200&endash;250 mcg a day can likely prevent mutation of latent, dormant retroviruses, including HIV, into virulent forms.137, 138, 139, 140, 141, 142, 143, 144, 145 This should lower and perhaps eliminate the risk of AIDS (acquired immune deficiency syndrome) among HIV-positive persons.
Dr Harold Foster argues:146 “The association of depressed CD4 T-cell counts and depleted plasma selenium stores is not coincidental. Rather, it provides evidence of the operation of a positive feedback system in which a fall in serum selenium triggers a reduction in the number of CD4 T-cells, which in its turn causes a further decline in serum selenium. This downward spiral undermines the immune system”–in what he dubs the “selenium-CD4 T-cell tailspin”. Accordingly, incidence of HIV/AIDS is high in areas of Africa where selenium in the soils is low, irrespective of people’s sexual behaviour.147, 148
Intramuscular injections of vitamin B12,149 supplements of vitamin E complex and N-acetyl-cysteine (NAC)150 also strengthen this AIDS defence. NAC seems to help replenish stores of reduced glutathione, lower inflammatory oxidative stress reactions and help protect against mitochondrial DNA damage, in turn decreasing replication of the virus.151, 152 Glutathione is humans’ chief internally generated antioxidant. The DNA in the mitochondria, the “power houses” of all our cells, has been described as 2,000 times more susceptible to oxidative damage than nuclear DNA.153 Adequate NAC serves further to facilitate detoxification in persons who have poor phase-II glucuronidation.154
Will Taylor, PhD, proposed a mechanism for selenium’s action. He is at the Computational Center for Molecular Structure and Design, Department of Medicinal Chemistry, University of Georgia. Dr Taylor sequenced the genetics of innocent, harmless retroviruses that normally lie dormant and cause no symptoms–retroviruses such as herpesvirus Simplex A, Coxsackievirus and HIV. (The usually benign character of HIV has been massively documented by Peter Duesberg, PhD, a leading retrovirologist at the University of California, Berkeley. To label HIV “the AIDS virus” or say that it “[always] causes AIDS” is wrong. Half of American AIDS patients are HIV-negative; and, as Dr Duesberg wrote in 1996, probably 90 per cent of the approx. 21 million HIV-positive people worldwide are healthy.155, 156)
Dr Taylor concluded that Coxsackievirus, HIV and certain other retroviruses are coded for the production of a selenoprotein; and he predicted that the selenoproteins produced by those viruses act as brakes on the viruses’ reproduction. In effect, with enough Se present, the HIV retrovirus makes its own “birth-control pill”. And so selenium has become very popular in HIV virus clubs.157 When there isn’t enough Se (the low level may not reflect inadequate dietary Se intake, Dr Taylor said), the virus goes wild. Supplemented selenium, even if the HIV can’t be eradicated, can effectively put it to sleep, preventing its conversion into AIDS.158
Coconut Oil
 Coconut oil, like mother’s milk, is rich in lauric acid, which the body converts to the antiviral fatty acid monolaurin. Dr Robert Atkins writes: “This may help in disarming a number of infectious viruses, including those that cause measles, herpes, Cytomegalovirus, vesicular stomatitis, and possibly AIDS.” However, Dr Atkins’s endorsement doesn’t extend to coconut milk, which contains too much sugar.159
Coconut oil, like mother’s milk, is rich in lauric acid, which the body converts to the antiviral fatty acid monolaurin. Dr Robert Atkins writes: “This may help in disarming a number of infectious viruses, including those that cause measles, herpes, Cytomegalovirus, vesicular stomatitis, and possibly AIDS.” However, Dr Atkins’s endorsement doesn’t extend to coconut milk, which contains too much sugar.159
(Excessive sugar intake is now recognised as the number one risk factor for heart attacks in women, and number two for men; excessive animal fat intake is number two for women, and number one for men.160 A major part of the explanation is this: just one teaspoon of sugar impairs the immune system by about 40 per cent for several hours, as Emanuel Cheraskin and associates found.161 Many Americans consume an average of two or more teaspoons of sugars of all kinds, every hour and all day, and thus keep their immunity constantly low. A very large number of heart attacks appear to be the result of infection, e.g., by H. pylori and Chlamydia pneumoniae.)
Mark Konlee, in his newsletter, Positive Health News, wrote about how coconuts saved an AIDS sufferer’s life:
“Chris, an AIDS sufferer, found his viral load had reached almost 700,000. He went for a relaxing vacation, packed all his drugs and headed for an Indian village in Surinam; there he dined on fresh coconut meat every day. Within two days his peripheral neuropathy was gone, and within two weeks he was ‘running through the jungle’.
“Back home, continuing to consume at least half of a coconut per day, his lab tests showed the viral load had dropped to just over 300,000. Within another month the viral load had dropped to non-detectable. ‘My doctor is completely baffled,’ said Chris.
“PPNF members may not be so puzzled. They read about the amazing health benefits of coconut, especially its antiviral characteristics, in Dr Mary Enig’s article in vol. 20 #1 of PPNF Health Journal in 1995.”162
Author’s Note:
This paper enlarges and updates my article on full-spectrum light, first published in Price-Pottenger Health Journal, Winter 1995, with added details, Spring 1995. Recent research, not yet incorporated into this paper, fully supports the statements made and conclusions here reached.
At the Da Vinci Holistic Health Center in Larnaca, Cyprus we use Full Spectrum Light for healing.
Endnotes:
1. Klapper JS. Documented health benefits of light. Townsend Letter for Doctors 1993(Apr):321-322.
2. Broad W, Wade N. Betrayers of the Truth: Fraud and Deceit in the Halls of Science. NY: Touchstone Books, 1982.
3. Ray DL, Guzzo L. Trashing the Planet. Wash., DC: Regnery Gateway, 1990.
4. Bland JS. Functional Med Update 1997 (Sept).
5. An example: a somewhat qualified researcher, who shields himself from sunshine at all times, expressed his disagreement to me in a letter. In it, he called me a “bastard” and a “liar”–both of which are inaccurate–and evidenced total loss of normal good manners. Then he returned my tactful reply letter, unopened.
6. Ceder K. Healthy office lighting: A bright idea. Healthy Office Rep 1992;2:3-4.
7. Kime Z. Sunlight. Penryn, CA: World Health Publ, 1980.
Downing D. Daylight Robbers. London: Arrow Books, 1988.
8. Hobday, Richard, The Healing Sun. Sunlight and Health in the 21st Century. Findhorn, Scotland, and Tallahassee, Florida: The Findhorn Press, 1999, pp. 42-43.
9. Schein OD, Vicencio C, Muoz B et al. Ocular and dermatologic health effects of ultraviolet radiation exposure from the ozone hole in southern Chile. Amer Jour Public Health 1995(Apr);85;4:546-550.
10. Lieberman B. Doomsday déjà vu: Ozone depletion’s lessons for global warming. Working paper, The European Science and Environment Forum, Cambridge, November 1998.
11. Moan J and Dahlback A. The relationship between skin cancers, solar radiation and ozone depletion. Brit Jour Cancer 1992:916-921.
12. Pearce F. Ozone hole innocent of Chile’s ills. New Scientist 1993(Aug 21):7.
13. Ridley M. Taking the sting out of the sunshine myth. The Sunday Telegraph 1994 (Apr 3).
14. JAMA 1998;280:714-718.
15. Black HS et al. Relation of antioxidants and level of dietary lipids to epidermal lipid peroxidation and ultraviolet carcinogenesis. Cancer Research 1985;45:6254-6259.
16. Bland JS. Func Med Update 2000 (Mar).
17. Leske MC, Chylack LT Jr, He Q et al. Antioxidant vitamins and nuclear opacities. Ophthalmology 1998;105:1,836.
18. Jacques PF et al. Long-term vitamin C supplement use and prevalence of early age-related lens opacities. Amer Jour Clin Nutr 1997;66:911-916.
19. Dr Ott made nearly all the time-lapse films for Disney; e.g., he compressed the growth, flowering and fruiting of a pumpkin plant into a minute or so on the viewer’s screen.
20. Ott, JN. Light, Radiation and You: How to Stay Healthy. Greenwich, CT: Devin-Adair Publishers, 1990.
21. Ott JN. Interview by Bland JS. Prev Med Update 1991 (Jan).
22. Am J Psychiatry 1991;146:9.
23. Garland FC et al. Occupational sunlight exposure and melanoma in the US Navy. Arch Environmental Health 1990;45:261-267.
24. The Politics of Sunlight. What Doctors Don’t Tell You 1995;5(12):12.
25. Peat R. Sunlight: Using it to sustain life. From Female Hormones (preprint, PO Box 5764 Eugene, OR 97405), 1995.
26. Rogers SA. Total Health in Today’s World 1997;2:4.
27. Peat R. op. cit.
28. Lee L. Your Health 1999(Jul);4(3):3.
29. Beral V et al. Malignant melanoma and exposure to fluorescent lighting at work. Lancet 1982(Aug 7):290-293.
30. Kustov VI et al. Epidemiology of malignant melanoma. Vopr Onkol 1987;33:35-39 (English abstract).
31. Lieberman B (Competitive Enterprise Institute, Washington, DC). Letter to Wall Street Journal, July 6, 1995.
32. Robinson B. Access to Energy, 1997 (various issues).
33. Kennedy AR et al. Fluorescent light causes malignant transformation in mouse embryo cell. Science 1980;207:1209-1211.
34. SAD no more &endash; Sunlight simulators lighten winter blues. Alternative Med 1998;26:14-16.
35. Ott JN. Interview by Bland JS, Prev Med Update 1991 (Jan).
36. Ott JN. Light, Radiation and You, op. cit.
37. Sunlamp use linked to melanoma. Sci News 1994;146:296.
38. Westerdahl J, Olsson H, Masback A et al. Use of sun lamps and malignant melanoma in southern Sweden. Am J Epidemiology 1994;140:691-699.
39. 20-20 TV show, 1996.
40. Valerian V. Leading Edge International Research Group. Release, Dec 21, 1998.
41. Prota G. Recent advances in the chemistry of melanogenesis in mammals. J Invest Dermatol 1980;75:122-127.
42. Rampen FH, Nelewans RT, Kerbeek ALM. Is water pollution a cause of cutaneous melanoma? Epidemiology 1992;3(3):263-265.
43. Douglass WC. Second Opinion 1994 (Feb).
44. Murray F. The Murray Report. Let’s Live 1997 (Oct 16).
45. It causes mutations, i.e., sudden variations in some inheritable characteristic in a germ cell of an individual animal (or person), as distinguished from a variation resulting from generations of gradual change.
46. Kurakawa Y, Takayama S et al. Long-term in vivo carcinogenicity tests of potassium bromate, sodium hypochlorite, and sodium chlorite conducted in Japan. Environ Cellular Perspectives 1996;69:221-25.
47. Meier JR. Genotoxic activity of organic chemicals in drinking water. Mutat Res 1988;196:211-245.
48. The prefix pheo- means “dusky”, “grey” or “dun”.
49. Cesarini J-R. Photo-induced events in the human melanocytic system: Photoagression and photoprotection. Pigment Cell Res 1988;1:223-233.
50. Rampen FH et al. Epidemiology 1992;3(3):263-265.
51. Murray F. The Murray Report. Let’s Live 1997 (Oct 16).
52. Hattersley JG. The negative health effects of chlorine. Jour Orthomolecular Med 2000;15(2):89-95.
53. Beral V, Ramchara S, Faris R. Malignant melanoma and oral contraceptive use among women in California. The Walnut Creek Contraceptive Drug Study. US National Institutes of Health, vol. III, 1986:247-252.
54. McCully KS. The Homocysteine Revolution: Medicine in the New Millennium. New Canaan, CT: Keats Publ, 1997.
55. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormone replacement therapy: Collaborative reanalysis of data from 51 epidemiological studies of 52,705 women with breast cancer and 108,411 women without breast cancer. Lancet 1997;350:1047-1059.
56. Lee JR. Natural Progesterone: The Multiple Roles of a Remarkable Hormone. California: BLL Publ, 1993.
57. Sellman S. Hormone Heresy: What Women MUST Know About Their Hormones. Honolulu, HI: GetWell International, 1998.
58. Sapolsky R. Interview by Bland JS, Funct Med Update 2000 (July).
59. Ott JN. Lecture to Society for Clinical Ecology, 1974.
60. Ott, JN. Light, Radiation and You, op. cit.
61. op. cit.
62. London, WP. Full-spectrum classroom light and sickness in pupils. Lancet 1987(Nov 21):1205-1206.
63. Calabrese, JR et al. Alternations in immunocompetence during stress, bereavement and depression; focus on neuroendocrine regulation. Am J Psychiatry 1987;14:1123-1134.
63a. Ott, JN. Light, Radiation and You, op. cit.
64. Finkel JS. New Eng J Med 1998 (March 19).
65. Ott JN. Lecture, op. cit.
66. Ott, JN. Light, Radiation and You, op. cit.
67. op. cit.
68. op. cit.
69. Rogers SA. Total Health in Today’s World 1997;1(2):2.
70. Ideal length of sun exposure is a personal matter and will depend in part on where you are. For myself, half an hour at midday without clothing is optimal in spring; 20 minutes in summer. This enables my body to accumulate a store of vitamin D3 for use during the fall and winter.
71. Ott, JN. Lecture, op. cit.
72. Peat R. Ray Peat’s Newsletter 1995;120:3.
73. Ott, JN. Lecture to Society for Clinical Ecology, 1974.
74. BIBIC Annual Report. British Institute for Brain Injured Children, Bridgewater, Somerset, England, 1997.
75. Dilman V, Dean W. The Neuroendocrine Theory of Aging and Degenerative Disease. Pensacola: Center for Bio-Gerontology, 1992:49,93-96.
76. Oxidation strongly linked to aging. Sci News 1993(Aug 14):109.
77. Oxidation strongly linked to aging. Sci News 1993(Aug 14):109.
78. Short RV. Melatonin: Hormone of Darkness, Brit Med J 1993;307:966-971.
79. Williams, David, DC. Pain and Sleep. What Doctors Don’t Tell You, Apr 2001.
80. Peat R. Ray Peat’s Newsletter 1995;120:3.
81. Wright JV, Gaby AM. Interview by Bland JS. Functional Med Update 1997 (Apr).
82. Webb RB. Genetic damage in Escherichia coli K12 AB2480 by broad-spectrum near-ultraviolet radiation. Science 1982;215:991-993.
83. Polz A. Personal communication, 1994.
84. Kripke DF. Light treatment for nonseasonal depression: Speed, efficacy, and combined treatment. J Affective Disorders 1998;49:109-117.
85. Thalen B-E et al. Light treatment in seasonal and nonseasonal depression. Acta Psychiatr Scand 1995;91:352-360.
86. The American way of death. Economist 1996(July 27):24.
87. Gloth FM III, Alam W, Hollis B. Vitamin D vs broad spectrum phototherapy in the treatment of seasonal affective disorder. J Nutr Health Aging 1999;3:5-7. In Sullivan K. The miracle of vitamin D. Price & Pottenger Nutrition Foundation. Wide Traditions 2000(Fall):11-20.
88. Ott JN. Interview by Bland JS. Prev Med Update 1991(Jan).
89. Kingham JD et al. Macular hemorrhage in the aging eye: The effects of anticoagulants. New Eng J Med 1988;3187:1126-1127 (letter).
90. Hattersley JG. Gain the benefits of aspirin without going blind. Health Freedom News 1998(Spring):34.
91. Mann D. Purple grape juice, wine and beer all cardioprotective. Med Tribune 1997(May 1):26.
92. Wright JV. Personal communication, 1995.
93. Seddon JM, Ajani UA et al. Dietary carotenoids, vitamins A, C, and E, and advanced age-related macular degeneration. Eye Disease Case-Control Study Group. JAMA 1994;272:1413-1420.
94. Hattersley JG. A sad note about ophthalmologists. Peer reviewed and submitted for publication, 1998.
95. Hattersley JG. Suggestions for avoiding macular degeneration. Townsend Ltr Doctors & Patients 1999(Feb/Mar):122-123 (letter).
96. Douglass WC. Second Opinion 1996 (June).
97. Cancer Research 1996;4108-4110.
98. Ainsleigh HG. Beneficial effects of sun exposure on cancer mortality. Prev Med 1993;12:132-140.
99. Sandyk R. Chronic relapsing multiple sclerosis. A case of rapid recovery by application of weak electromagnetic fields. Int J Neurosciences 1995:82. Sandyk R. Reversal of alexia in multiple sclerosis by application of weak electromagnetic fields. Int J Neurosci 1995:82.
100. Sandyk R. Zinc deficiency in attention-deficit hyperactivity disorder. Int J Neurosci 1990;52:239-241 (letter).
101. Aldegunde M, Miquez I, Veira J. Effects of pinealectomy on regional brain serotonin metabolism. Int J Neurosci 1985;26:9-13.
102. Kruesi MJ, Rapaport JL, Hamburger S et al. Cerebrospinal fluid monoamine metabolites, aggression, and impulsivity in disruptive behavior disorders of children and adolescents. Arch Gen Psychiatr 1990;47:419-426.
103. Toren P, Eldar S, Sela B-A, Wolmer L et al. Zinc deficiency in attention-deficit hyperactivity disorder. Biol Psychiatry 1007;40:1308-1310.
104. Science News 1992(Aug 8);144:109.
105. Life Extension Foundation. Life Extension Update 1993 (June).
106. Oxidation strongly linked to aging. Sci News 1993(Aug);14:109.
107. Kerenyi NA, Pandula E, Feuer G. Why the incidence of cancer is increasing: The role of light pollution. Med Hypotheses 1990;33:75-78.
108. Dilman V, Dean W. The Neuroendocrine Theory of Aging and Degenerative Disease. Pensacola, Florida: Center for Bio-Gerontology, 1992;49:93-96.
109. Sandyk Reuven. Interview by Bland JS, Prev Med Update 1996 (Dec).
110. Grimes DS. Sunlight, cholesterol and coronary heart disease. Quarterly J Medicine 1996;89:579-589.
111. Rall LC, Meydani SN. Vitamin B6 and immune competence. Nutr Rev 1993;41:217-225.
112. Hattersley JG. Vitamin B6: The overlooked key to preventing heart attacks. Jour Applied Nutr 1995;47:24-31.
113. Spencer FA et al. Seasonal distribution of acute myocardial infarction in the Second National Registry of Myocardial Infarction. Jour Amer Coll of Cardiology 1998(May);31(6):1226-1233.
114. Grimes D. Interview by Kirk Hamilton, PA-C, The Experts Speak. Clinical Pearls News 1997(Sept);7(9):99,109-111.
115. Hypertension 1997;30:150-156.
116. Recer P. Sun may prevent breast cancer. Seattle Post-Intelligencer 1997(Nov 4):A1,A4.
117. Wang ZY, Huang MT, Lou YR, et al. Inhibitory effects of black tea, green tea, decaffeinated black tea, and decaffeinated green tea on ultraviolet B light-induced skin carcinogenesis in 7,12-dimethylbenz[a]anthracene-initiated SKH mice. Cancer Res 1994;54:3428-3435.
118. Conney AH, Wang Z-Y, Huang M-T et al. Inhibitory effect of green tea on tumorigenesis by chemicals and ultraviolet light. Prev Med 1992;21:361-369.
119. Ahmad N, Feyes DK, Nieminen A-L, Agarwal R, Mukhtar H. Green tea constituent epigallocatechin-3-dallate and induction of apoptosis and cell cycle arrest in human carcinoma cells. J Natl Cancer Inst 1997;89:1881-1886.
119a. Andreas Schuld, [email protected] or [email protected].
120. Examples include grape skins, grape seeds (if chewed up), and the tasteless white pulp inside citrus peels.
121. Imai K, Nakachi K. Cross-sectional study of effects of drinking green tea on cardiovascular and liver diseases. Brit Med Jour 1995;310:693-696.
122. Opara EC. Antioxidants &endash; The latest weapon in the war on smoking, Part 2. VRP Nutritional News 1997;11(8):4,10.
123. Sternberg S. Breathing freely threatens seeing clearly. Sci News 1997(Mar 8);151:143. See also JAMA 1997 (Mar 5).
124. Wright JV. Interview by Bland JS. Funct Med Update 1997 (Apr).
125. Cunnane SC et al. Nutritional attributes of traditional flax-seed in healthy young adults. Am J Clin Nutr 1995;61:62-68.
126. Bland JS. Prev Med Update 1995 (Apr).
127. Journal of Nutrition 1997;127;3:544-548.
128. Budwig J. Flax oil as a true aid (lecture, 1959). In Budwig J. Flax Oil as a True Aid Against Arthritis, Heart Infarction, Cancer and Other Diseases. Vancouver, BC: Apple Publ, 1992.
129. Jang M et al. Cancer chemopreventive activity of resveratrol, a natural product derived from grapes. Science 1997;275:218-220.
130. Peat R. Coconut oil. In Mercola J. eHealthy News You Can Use 2001 (Mar 24).
131. HealthNotes 1997 (Sept).
132. J Amer Acad Dermatology 1998;38:45-48.
133. Bland JS. Funct Med Update 1997 (Apr).
134. Foster H. Sudden infant death syndrome: The Bradford Hill criteria and the evaluation of the thyroxine deficiency hypothesis. J Orthomolecular Med 1993;8(4):201-227.
135. Smith LH with Hattersley JG. Victory over crib death. Townsend Letter for Doctors & Patients 2000(Aug/Sept):50-54, 126-131.
136. Smith, Lendon H, MD, with Hattersley Joseph, MA. The Infant Survival Guide: Protecting Your Baby from the Dangers of Crib Death, Vaccines, and Other Environmental Hazards. Petaluma, CA: Smart Publications, 2000.
137. Dworkin BM. Selenium deficiency in HIV infection and the acquired immunodeficiency syndrome (AIDS). Chem-Biol Interactions 1994;91:181-186.
138. Gaby AM, Wright JM. Interview by Bland JS. Funct Med Update 1997 (Apr).
139. Altavena C, Dousset B et al. Relationship of trace element, immunological markers, and HIV-1 infection progression. Biol Trace Elem Res 1995;47:133-138.
140. Passwater RA. Vitamin connection. More exciting research from Dr Will Taylor. Selenium against viruses. Whole Foods 1996;19(11):133-138.
141. Taylor EW, Bhat A et al. HIV-1 encodes a sequence overlapping env gp41 with highly significant similarity to selenium-dependent glutathione peroxidases. J AIDS Hum Retrovirol (in press).
142. First International Symposium on Human Viral Diseases: Selenium, Antioxidants and Other Emerging Strategies of Therapy and Prevention. April 19-21, 1996. Nonnweiler, Germany. Int Antiviral News 1996;4(5):84-86.
143. Taylor W. Selenium and viral diseases: Facts and hypotheses. Computational Center for Molecular Structure and Design. Dept of Medicinal Chemistry, University of Georgia.
144. Look MP, Rockstroh JK et al. Serum selenium and erythrocyte glutathione peroxidase in human immunodeficiency virus-1 infection. Biol Trace Elem Res 1996 (in press).
145. Taylor EW, Nadimpalli RG, Ramanathan CS. Genomic structures of viral agents in relation to the biosynthesis of selenoproteins. Biol Trace Elem Res. Symposium Volume. Schrauzer G, Montagnier L, eds (in press).
146. Foster HD. AIDS and the “selenium-CD4 T-cell tailspin”. The geography of a pandemic. Townsend Ltr Doctors & Patients 2000(Dec):94-99.
147. Harvard AIDS Institute web page, http://www.hsph.harvard.edu/hai/interactive/map-africa.html.
148. Howe MG. International variations in cancer incidence and mortality. In Global Geocancerology: A World Geography of Human Cancers (Howe GM, ed.). NY: Churchill Livingston, 1986:3-42.
149. Levander OA, Ager AL, Beck MA. Vitamin E and selenium: Contrasting and interacting nutritional determinants of host resistance to parasitic and viral infections. Proc Nutr Soc 1995;54(2):475-487.
150. Notter HS, Moelans II, de-Vos NM, de Graaf L, Visser MR, Verhoef J. N-acetyl-cysteine-induced upregulation of HIV-1 gene expression in monocyte-derived macrophages correlates with increased NF-KB DNA binding activity. J Leukocyte Biol 1997;61;1:33-39.
151. Bland JS. Funct Med Update 1997 (Dec).
152. Rivabene R, Straface E, Giammarioli AM, Rainaldi G, Malorni W. Combined effect of 3-aminobenzamide and N-acetylcysteine on HIV replication in chronically infected U937 cells. Redox Rep 1997;3(3):145-151.
153. Ames B. Cited on Bland JS. Funct Med Update 1997;Dec.
154. O’Grady JG. Paracetamol hepatotoxicity: How to prevent it. J Royal Soc Med 1997;90(1):368-370.
155. Duesberg D. Inventing the AIDS Virus. NY: Regnery, 1996.
156. Hattersley JG. The AIDS scam. Unpublished document, 1997, approved by Dr Duesberg.
157. Wright JV, Gaby AM. Interview by Bland JS. Funct Med Update 1997 (Apr).
158. Taylor EW. Interview by Bland JS. Funct Med Update 1997 (May).
159. Atkins R. A nutritional paradise in ‘forbidden oils’. Dr Robert Atkins’ Health Revelations 1997;5(12):6-7.
160. Grant WB. Reassessing the role of sugar in the etiology of heart disease. J Orthomolecular Med 1998;13(2):95-104.
161. Wright JV. Preventing colds, flu and infection: Plan ahead to fight off germs for this fall’s season of sickness! Dr Jonathan V. Wright’s Nutrition & Healing 2001;8(4):1-3.
162. Health Vectors, PPNF Health Journal 1997;21(2):6-7.
About the Author:
Joseph G. Hattersley in 1953 completed everything then required for a PhD degree in economics, except a dissertation, at the University of California, Berkeley. In 1976, at age 54, a seeming nutritional miracle launched his career of writing on a wide range of health topics. Joe seeks to integrate differing views on a subject from competing research teams. Several of his proposals have been confirmed three to five years later in mainstream medical and scientific journals. His special interests are prevention of heart disease and cot death. His article, “Soybean Products: A Recipe for Disaster”, was published in NEXUS 4/03, April&endash;May 1997 issue.
Extracted from Nexus Magazine, Volume 8, Number 4
PO Box 30, Mapleton Qld 4560 Australia. [email protected]
Telephone: +61 (0)7 5442 9280; Fax: +61 (0)7 5442 9381
From our web page at: http://www.nexusmagazine.com/
[Editor’s Note: This article refers to several research studies involving animals. We wish to advise that NEXUS does not condone animal experimentation or vivisection.]